
 – Primary thrombocythemia ( myeloproliferative disorder)")
Case study (32) – Primary thrombocythemia
( myeloproliferative disorder)
A 76-year-old woman has a history of gradual coldness and numbness in her fingertips for 2 to 3 months.
The symptoms are persistent but episodic.
She is a non-smoker.
Her feet are normal, and her physical examination is normal.
All pulses are present.
CBC:
Hemoglobin (Hb) 90 g/L
White blood cells (WBC) 14.6 X 109/L (neutrophils 67%)
Platelets 1246 X 109/L
Questions:
Q1. Comment on the appearance of the hands.

Q2. Comment on the blood film.

Q3. What are the possible causes of abnormalities?
Q4. What further investigations would you undertake?
Q5. What are the possible treatments?
Answers:
A1. Severe ischemic changes are affecting the hand.
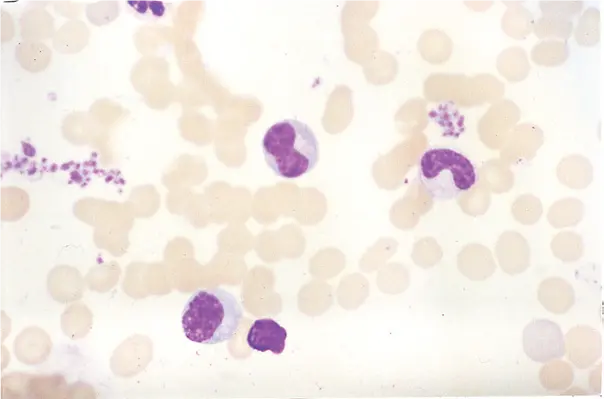
A2. The blood film shows increased numbers of circulating platelets, with marked platelet anisocytosis and many giant platelets.
A3. Increased platelets may be primary or secondary.
Primary thrombocythemia turned out to be the diagnosis in this case, and this is a myeloproliferative disorder; a raised platelet count is also encountered as part of other myeloproliferative disorders, for example, chronic granulocytic leukemia, polycythemia vera.
Secondary thrombocytosis is due to Infection, bleeding, iron deficiency, and malignant tumors can be seen after splenectomy.
A4. A full history and physical examination are needed to exclude causes of secondary thrombocytosis.
A bone marrow aspirate with chromosome analysis and a trephine biopsy may confirm primary thrombocythemia.
About 50% of patients with essential thrombocythemia (ET) have mutations in the Janus kinase 2 (JAK2) site (V617F), and a High proportion
Among JAK2-negative patients, there is a mutation at the CALR locus.
Serum ferritin is needed to rule out iron deficiency, and abdominal ultrasound may reveal an enlarged spleen.
Platelet function tests are typically abnormal in primary thrombocythemia and normal in secondary or reactive states.
A5. Primary thrombocythemia is treated with chemotherapy (e.g. oral hydroxyurea) to lower the platelet count and maintain it below 400 × 109/L, and antiplatelet therapy (e.g. aspirin 150 mg every second day) to inhibit platelet function.
The figure below shows increased platelet numbers in association with abnormal, hypogranular neutrophils. This patient has myelodysplasia; cytogenetic analysis shows the presence of 5q–, which is related to slowly proliferating myelodysplasia and macrophages and thrombocytosis.
The figures below illustrate the JAK2 assay and the calreticulin (CALR) assay

Janus kinase 2 (JAK2) assay is an amplification refractory mutation system polymerase chain reaction (PCR). The wild type (WT) allele produces two bands, while the mutant (MT) allele produces three bands.

Calreticulin (CALR) assay. There are more than 30 different mutations in the 9th exon of this gene, all of which will produce the same frameshift and abnormal 3'protein. The PCR products were examined by capillary gel electrophoresis. The wild-type allele band is 263 bp.
 – Primary thrombocythemia ( myeloproliferative disorder) A 76-year-old woman has a history of gradual coldness and numbn…){kind=link}
Comments
Post a Comment